Continuous or intermittent fetal monitoring: Which is recommended during labor?
Updated: 27/03/2017
What is the origin of fetal auscultation?
The origin of fetal monitoring comes from the early 19th century when the fetal heartbeat began to be listened to diagnose intrauterine life. The first signs of fetal auscultation consisted of placing the ear on the woman's abdomen. Later, the first stethoscopes began to appear, but it was not until 1876 that the Pinard stethoscope emerged. [1]

Pinard Stethoscope
During the 19th century, interest began to grow in identifying heart rate patterns indicative of fetal well-being, and by the early 20th century, fetal auscultation was already an established practice in Europe [2].
The first fetal electrodes emerged in 1960, four years later the Doppler effect was detailed, and in 68 the first electronic fetal monitor was invented [1].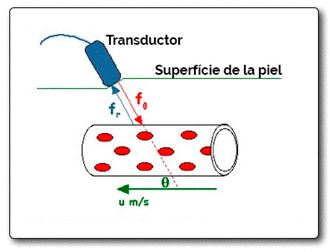
Sonography: Illustration of blood flow detection through the Doppler effect. Based on a public domain image by Kieran Maher (see original image)
The auscultation of the fetal heart rate is so important because it allows detecting fetuses at risk, so it is key to control the health of the fetus [1].
Continuous fetal monitoring versus intermittent monitoring
Continuous fetal monitoring, which was introduced in the 50s in delivery rooms, has been linked to an increase in cesarean sections and operative vaginal births [3][4].
Based on this, numerous clinical trials [5][6][7] have studied intermittent auscultation versus continuous, to evidence which is the most recommended technique during labor with low-risk pregnant women.
According to the most recent literature, in a low-risk delivery, being a healthy woman, without medical complications in pregnancy, intermittent monitoring is advised. On the other hand, continuous auscultation is associated with an increase in instrumented births, and a large increase in the rate of cesarean sections [8][9][10].
The advantage of intermittent auscultation is that it does not limit the woman's mobility, so the fact of being able to adopt different positions in delivery, results in a better tolerance of pain, less use of epidural anesthesia, reduction of the dilation period, among other things [11][12].
When to practice continuous fetal monitoring?
According to numerous studies, there is a correlation between high-risk pregnancies, and the onset of neonatal encephalopathies, cerebral palsy, and perinatal death [13][14] , therefore in this case continuous fetal monitoring is highly recommended.
Conclusions
In order to put the most suitable option into practice, professionals must know what the most recent scientific evidence is.
In conclusion, according to the conclusions gathered in the cited review [15] , continuous fetal auscultation should not be applied in low-risk pregnancies, as it tends to increase the rate of cesarean sections and instrumented births.
Looking for a fetal monitor?
At DH Medical Material we recommend the BT350 fetal monitor with LED screen. Get it on offer until May 1st with the Gynecology Special from 1,195.00 €, before 1,259.00 €.
•7-segment LED screen
•Data handling of 150 patients
•Detection of fetal movement and contraction
•Waterproof probes
•FHR range: 30 - 240 FHR
•Doppler sound alarms
Do you have any questions about which fetal monitor to choose? You can consult us through the following link or by calling us at 93 864 37 07 or writing to info@dhmaterialmedico.com.
Bibliography
[1]. Royal College of Obstetricians and Gynaecologist. The Use of Electronic Fetal Monitoring. The use of interpretation of cardiotopography in intrapartum fetal surveillance. London: Royal College of Obstetricians and Gynaecologist, 2001.
[2]. Gillmer MD, Combe D. Intrapartum fetal monitoring practice in the United Kingdom. BJOG. 1979; 86: 753-8
[3]. Neilson JP, Lavender T, Wray S, Quenby S. Obstructed labour: reducing maternal death and disability during pregnancy. Br Med Bull. 2003; 67: 191-204
[4]. Vintzileos AM, Antsaklis A, Varvarigos I, Papas C, Sofatzis I, Montgomery JT. A randomized trial of intrapartum electronic fetal heart rate monitoring versus intermittent auscultation. Obstet Gynecol. 1993; 81: 899-907.
[5]. Vintzileos AM, Antsaklis A, Varvarigos I, Papas C, Sofatzis I, Montgomery JT. A randomized trial of intrapartum electronic fetal heart rate monitoring versus intermittent auscultation. Obstet Gynecol. 1993; 81: 899-907
[6]. MacDonald D, Grant A, Sheridan-Pereira M, Boylan P, Chalmers I. The Dublin randomized controlled trial of intrapartum fetal heart rate monitoring. AJOG. 1985; 152: 524-39.
[7]. Haverkamp AD, Orleans M, Langerdoerfer S, McFee J, Murphy J, Thompson HE. A controlled trial of the differential effects of intrapartum fetal monitoring. AJOG. 1979; 134: 399-412.
[8]. Luthy DA, Shy KK, Van Belle G. A randomized trial of electronic fetal monitoring in preterm labor. Obstet Gynecol. 1987; 69: 687-95.
[9]. Wood C, Renou P, Oats J, Farrell E, Beischer N, Anderson I. A controlled trial of fetal heart rate monitoring in a low-risk obstetric population. AJOG .1981; 141: 527-34.
[10]. Haverkamp AD, Orleans M, Langerdoerfer S, McFee J, Murphy J, Thompson HE. A controlled trial of the differential effects of intrapartum fetal monitoring. AJOG. 1979; 134: 399-412.
[11]. MIDIRS and NHS Centre for Reviews and Dissemination. Informed choice for professionals: positions in labour and delivery. Bristol: MIDIRS, 2004.
[12]. Gupta JK, Hofmeyr GJ. Position for women during second stage of labour. Cochrane Review. The Cochrane Library, Issue 3, 2004. Oxford: Update Software.
[13]. Nelson KB, Ellenberg JH. Antecedents of cerebral palsy. Multivariate analysis of risk. N Engl J Med. 1986; 315: 81-6
[14]. Adamson SJ, Alessandri LM, Badawi N, Burton PR, Pemberton PJ, Stanley F. Predictors of neonatal encephalopathy in full term infants. BMJ. 1995; 311: 598-602.
[15]. Jiménez M., Pérez Anna. The use of fetal monitoring during labor in low-risk pregnant women. Matronas Pro. 2008; 9 (2):5-11

